



 Publications
Publications
 Partners
Partners





- Diabetes is the second leading cause of death in SA after tuberculosis, according to Statistics South Africa.
- There is, however, no clear picture as to how many people have diabetes or how many people are receiving diabetes care.
It leaves the health system ill-equipped to handle the growing diabetes crisis.
While surveys have shed some light on diabetes prevalence in South Africa, inconsistency in survey approaches and an over-reliance on self-reporting measures - as opposed to objective blood-based biomarkers - make it difficult to determine how many people actually have the disease.
The most widely cited figure is 4.2 million. This is the number of people that the International Diabetes Federation (IDF) estimated as living with diabetes in the country in 2021.
Yet, the IDF's estimate is not drawn from data generated in South Africa, but inferred from data from Tanzania - a country with a very different health profile from South Africa.
Percept, a consulting firm based in Cape Town, has produced alternative estimates derived from local data, including available population surveys and medical schemes data. This arguably paints a more accurate picture of the reality in South Africa.
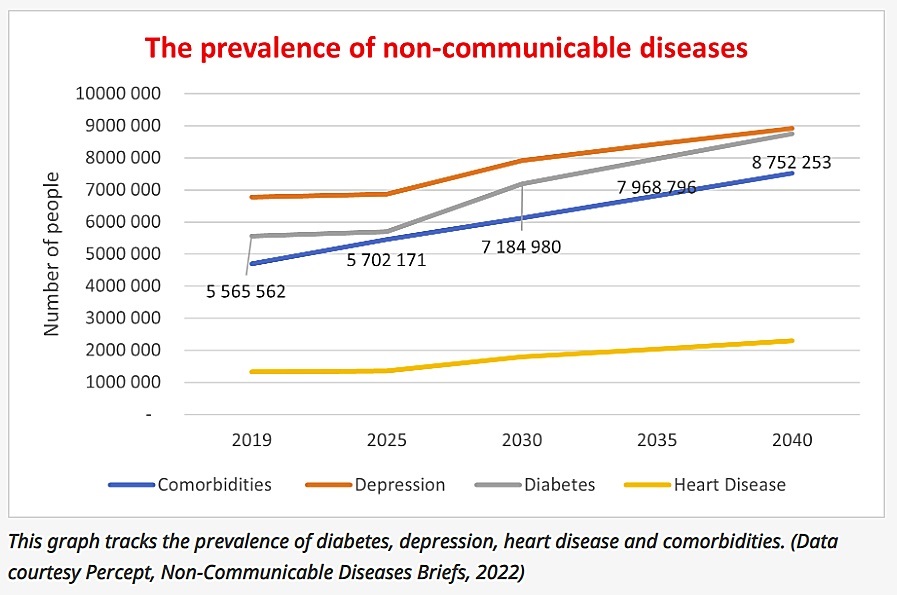
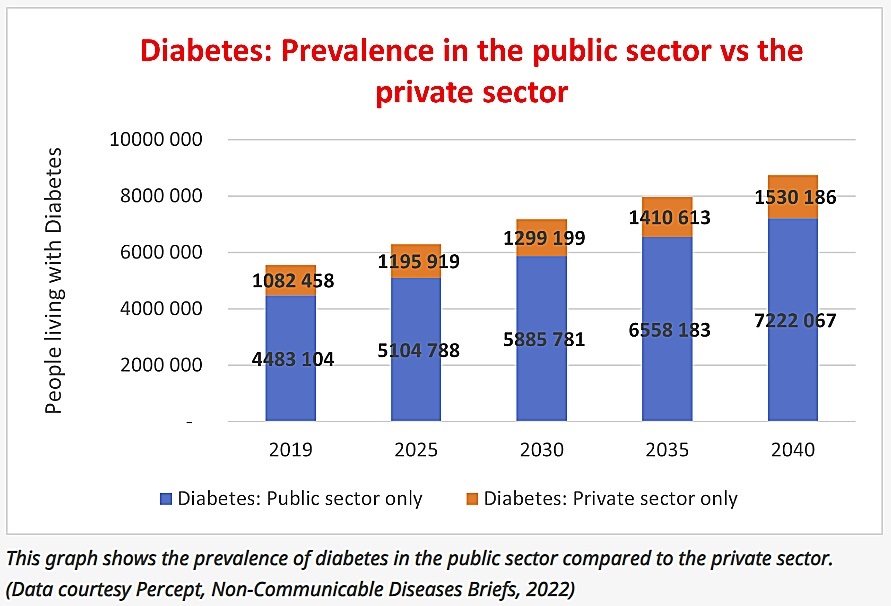
Percept estimates that just under 5.6 million people were living with diabetes in South Africa in 2019 - 80% of whom accessed healthcare in the public sector.
For comparison, around 7.8 million people in the country were living with HIV in 2023, according to the latest estimates from Tembisa, the leading mathematical model of HIV in South Africa.
Percept forecasts that, like many other countries, South Africa is predicted to see ballooning numbers of diabetes cases in the coming decades – rising to an estimated 8.75 million in 2040.
While the government has committed to scale-up interventions to tackle diabetes in its 2022-2027 National Strategic Plan (NSP) on Non-Communicable Diseases (NCDs), little progress has been made in establishing the monitoring and surveillance systems that will tell us whether the requirements are being met.
"People are dying of something that nobody should ever have to die from, and we don't know where they are, we don't know if they're getting care, and we don't know if they're getting medicine," Sweet Life's Bridget McNulty told Spotlight.
Sweet Life is a community of people living with diabetes that focuses on empowering people living with the condition.
What types of data do we need?
Firstly, we need up-to-date data on how many people in the country have or are at risk of developing diabetes. This data could be collected through large surveys that are regularly repeated and comparable over time. South Africa, for example, has such an HIV survey that is run roughly every five years.
Bilqees Sayed, Deputy Director at the National Department of Health, told participants at a Diabetes Summit in November last year that South Africa was considering implementing the World Health Organisation (WHO) STEPwise approach to gather information on NCD risk factors.
This approach includes, among other elements, execution of a household survey in which blood samples are collected through a finger prick to measure participants' blood glucose levels.
The National Department of Health, however, did not respond to questions from Spotlight on its plans for implementing such surveys.
Secondly, South Africa needs better data to tell us how many people with diabetes are dying and what they are dying from (people with uncontrolled diabetes may die from heart disease, stroke, or other diabetes-related causes).
Statistics South Africa has published mortality data generated from cause of death notifications up to 2018.
This data shows a worrying rise in the number of people dying of diabetes over the past decade. However, there is concern that the way that data is captured in death notifications fails to properly reflect the extent to which diabetes contributes to deaths.
As with HIV, diabetes might in some cases be a contributing factor to someone's death, but not be noted on a person's death certificate.
And, thirdly, South Africa needs better routinely captured data to understand people's journey through the healthcare system. Who is at risk of diabetes? Who has been screened? Who has been diagnosed? Who has been linked to care and how are they fairing?
Outside of the Western Cape, where the provincial health department has developed digital systems for tracking people's health data, very little such routine monitoring of diabetes is done.
Why do we know so little about diabetes in SA?
One reason is that much of the country's health systems focus, political will, and investment over the last two decades has been directed towards addressing HIV and TB. This is understandable. There was a real and urgent need for the country to respond to the dual HIV and TB crises. International donors were also keen to provide funding to combat these diseases.
While South Africa has made significant progress in improving care and strengthening monitoring and surveillance for HIV and TB, this has rarely trickled down to support other disease responses.
Consider how patient folders are managed. When patients are seen at a primary care clinic for HIV or TB, their folders go into a special pile for facility-based data capturers to upload relevant HIV and TB information into a national digital system.
These digitisation efforts have provided the country with rich data on how many people have been diagnosed with HIV and/or TB, where they are, who they are, whether they are on treatment, and how well they are doing on treatment.
But if a patient is seen at a clinic for diabetes, their data typically never moves beyond the paper-based patient folder in which it is recorded. While this should at the very least allow for the continuity of care when someone repeatedly visits the same health facility, patient folder management systems in primary clinics are notoriously wonky - with folders often going missing or patient confidentiality being put at risk.
Another difference between HIV and TB and diabetes is the use of registers - primary clinics have long used paper-based registers (with carbon copy pages that can be removed for monitoring purposes) to keep track of patients diagnosed and/or treated for HIV and TB at their facilities.
While the National Department of Health's 2014 guidelines for primary care level management of Type 2 diabetes state that clinics should maintain a register of people living with diabetes to allow for recall of patients when necessary, this recommendation remains unimplemented (except in a few clinics that took the initiative to do this on their own).
READ | Diabetes, heart disease, cancers on the rise, as South Africans are urged to prioritise health
Without digitised data on the interactions of people with diabetes with the health system, or clinic-based registers, the only way to identify diabetes patients at most health facilities is to conduct a full audit of all the patient folders at a facility. These types of time-consuming audits have been done in some locations for academic purposes. The results were disheartening.
"We found facilities where the filing system had completely collapsed," Dr Patrick Ngassa Piotie, the chairperson of the Diabetes Alliance and co-founder of the University of Pretoria's Diabetes Research Centre, told Spotlight of the centre's experience auditing medical files at primary clinics.
He added:
The lack of systems to track and recall patients with diabetes can put lives at risk. During the height of the Covid-19 pandemic, the absence of such systems hamstrung efforts by NGOs and the government to target messaging and interventions at this group. People with diabetes face a higher risk of severe-illness or death from Covid-19 than people without diabetes.
How the Western Cape has shot ahead
Over the past two decades, the Western Cape health department worked to develop a Provincial Health Data Centre (PHDC) that collates data from several data sources. The system brings together data on facility visits, hospitalisation, diagnostic lab results, and the dispensing of medication. In addition to allowing the province to better track health outcomes at a provincial level, the system allows for continuity of care across the province.
Dr Muzzammil Ismail illustrated to Spotlight, over Zoom, how health providers in the province can infer when a person was diagnosed with diabetes (from lab results or medicine dispensing data), what medicines they have been given, how controlled their diabetes is over time, and whether they have been hospitalised with a diabetes-related complication, all using an innovative online tool.
The system also allows healthcare providers to see what other conditions a person has been diagnosed with and is receiving treatment for.
Ismail tells Spotlight that, while the provincial data system enables monitoring and research, its primary purpose is "to support clinical decision-making for how you actually care for patients".
Can the National Department of Health establish similar systems?
While the Western Cape's system has been developed using open-source computer programmes that could be adopted by other provinces and nationally, the National Department of Health has opted to develop its own systems instead.
President Cyril Ramaphosa announced in February 2023 that "using the capabilities of the electronic vaccination record system we developed for Covid-19, the Department of Health will introduce an Electronic Health Record solution to improve management of health records".
Similarly to the Western Cape's system, the Electronic Health Record system will seek to link patient data under a unique identifier or patient registration system. Much like an ID number, a unique identifier is a number or code that links health records to a specific? individual.
The timeline for implementation of this Electronic Health Record - which has been touted as a necessary step toward National Health Insurance - is unclear.
The National Department of Health did not respond to questions regarding the timeline for implementing the Electronic Health Record system by publication of this article (though it did last year answer several questions from Spotlight on the government's new health information system).
ALSO READ | Can you get diabetes from eating too many sweets? Dietitian separates fact from fiction
How well the department can implement an Electronic Health Records system and how long this will take remains to be seen. The availability of relevant digital skills and infrastructure across the country is limited and, apart from the Western Cape, the track-record of the last two decades is not inspiring.
Diabetes and NCD advocates argue that when the Electronic Health Record System is implemented, its initial implementation should not prioritise monitoring of HIV and TB over other conditions.
Sandhya Singh, NCD policy activist and a former director in the NCD cluster at the National Department of Health, says that "the electronic health record system should be implemented as soon as possible to benefit all people irrespective of their condition".
She adds:
Another area of uncertainty is the stalled establishment of the National Public Health Institutes of South Africa (NAPHISA).
In short, the vision with NAPHISA was to create a new entity that would be tasked with helping the country get to grips with growing health threats like diabetes.
Currently, the National Institute of Communicable Diseases (NICD), located in the National Health Laboratory Services (NHLS), is - to some degree - also supporting the monitoring of non-communicable diseases (see for example, the Cancer Registry). However, it is anticipated that monitoring of NCDs will fall under the domain of NAPHISA once it is established.
But, while the legislation to set up NAPHISA was passed in 2020, the entity has not yet been established, nor are there any indications that it will be soon.
What can be done now?
While we wait for the new Electronic Health Record system to be developed and for NAPHISA to be established, we can set several other balls rolling.
To start with, we could act on the relevant WHO recommendations.
As noted above, Sayed told participants at the 2023 Diabetes Summit that the National Department of Health is considering implementing the WHO's STEPwise approach, which would include a household survey component that measures diabetes risk and collects blood glucose measurements.
In addition, Mzi Gcukumana, senior communications manager at the NHLS, told Spotlight that the health department is working with the WHO to roll out the integrated disease surveillance system (IDSR), and this system includes reporting new cases of diabetes.
These are positive signs, but as with any such promises or undertakings, the proof of the pudding will be in the eating.
Second, the health department could include more diabetes indicators in its existing digital data systems – most notably in the District Health Information System (DHIS).
The DHIS collects data on multiple indicators, including for example cervical cancer screenings and maternal and child health outcomes, from public health facilities across the country. However, efforts to include diabetes indicators on the DHIS have had limited success to date.
READ MORE | Stigma, inaction and cost: Will SA treat obesity with lessons learned from HIV?
Sayed told participants at the 2023 Diabetes Summit that "we do not have an integrated electronic system for NCD surveillance at the national level [and] we rely on the DHIS, which is not appropriate in terms of the number of data elements and indicators that are being collected for NCDs".
She added: "It is a constant battle to have our data being included onto the DHIS."
While the DHIS should ideally monitor indicators for secondary complications related to diabetes, Sayed noted, "unfortunately when these are proposed to our M&E [monitoring and evaluation] people and presented to provinces, we are told that these indicators and data elements cannot be included because we do not have a register which collects this data".
Third, we could establish a national diabetes registry.
To do this, we'd have to figure out what types of data need to be collected at what levels of care. TB registries, for example, collate patient data from facilities to enable recall of patients (this approach was recommended in the Department of Health's 2014 guidelines for diabetes, but never implemented).
Alternatively, the National Cancer Registry is collated from laboratory data.
Gcukumana tells Spotlight that if a diabetes registry is created, it's primary purpose "should be to support improvement in the quality of care and adherence to national and international treatment guidelines", adding that "it will require collating laboratory and patient data: blood glucose, HbA1c, creatinine, urine albumin, age, weight, height, BP, prescribed medication and eye test results".
Diabetes advocates, however, said the health department was resistant to creating a diabetes-specific registry due to concerns that this would further entrench the silo-ed approach to healthcare that arose in response to HIV and TB, which the department was now trying to move away from.
READ | One in four people with HIV not on treatment - new estimates
In the absence of a national registry, the Diabetes Alliance, the University of Pretoria, and partners have begun exploring opportunities to create a Type 1 diabetes registry through field research, as well as creation of an online platform that allows people to submit their own information to be counted on the registry.
Such a patient-led cancer registry was recently launched in South Africa. (While 90% of people with diabetes have Type 2 diabetes, around 10% of people with diabetes have Type 1. Type 1 diabetes, which typically appears in children, is generally managed by specialists at hospitals).
Lastly, we can make better use of the extensive laboratory infrastructure at the NHLS. People with diabetes receiving care through the public sector should at minimum be receiving an HbA1c blood test once a year.
The results of this test tell people with diabetes and their healthcare workers how well controlled their diabetes is. The NHLS houses all the laboratory data for the estimated 80% of the population that access diabetes care through the public sector.
Gcukumana told Spotlight the NHLS had HbA1c and creatinine data from tests performed in the public sector.
He added that some of this data had already been analysed and published, while other analyses were ongoing.
The seeds were thus there, but such work-ups and its collation into useful statistics should become at least as common as viral load tests and data for HIV.
'You can't improve what you can't measure'
Despite the various uncertainties regarding the data, most experts agree on the broad premise that diabetes rates will only increase in the coming decades.
At the same time, with the development of new classes of diabetes medicines, such as GLP-1 agonists (semaglutide and so on), we have new options for treating diabetes and weight problems early, and if treating early enough, potentially preventing it.
If we get it right, there is the potential in the coming years to save many lives and save many people the hardships that often come with diabetes.
But delivering on that potential brings us back to where we started this special briefing.
South Africa has adopted several good targets to improve diabetes care and outcomes under the relevant strategic plan.
But we lack baseline measurements of our performance against those targets.
The pockets of data that we have from academic research show that even where people are being diagnosed with diabetes and linked to care they are often faring poorly, experiencing poorly controlled blood sugar levels and debilitating complications.
But that is only a part of the picture. The harsh reality is that much of the suffering due to diabetes remains hidden.
Ultimately, it is quite simple. As McNulty says: "You can't improve what you can't measure."
*This special briefing is part of a series by Spotlight – health journalism in the public interest. Sign up to the Spotlight newsletter.





















